




























http://www.freepressjournal.in/analysis/rn-bhaskar-the-abject-state-of-medicare-in-india/1008722
India’s Medicate — terrible state; forgotten objectives
How does medicare fare in India? The blunt answer is that nobody really knows. There is very little data available. Or at least, if the data is available with the government, little goes out to global organizations like WHO (World Health Organisation) where data is captured for comparison.
India used to do a better job of data collation and dissemination till 1991 – at least that is what the WHO data sheets suggest (State of medicare – WHO data – http://apps.who.int/gho/athena/data/GHO/HRH_26,HRH_33,HRH_28,HRH_25,HRH_27,HRH_31,HRH_29,HRH_30,HRH_32.html?profile=ztable&filter=COUNTRY:*). The chart given alongside shows how India was more efficient in providing data to the WHO in 1991 than it is today. Most fields are shown as blanks, indicating that the government does not have the data, or at least has not communicated this to the WHO.
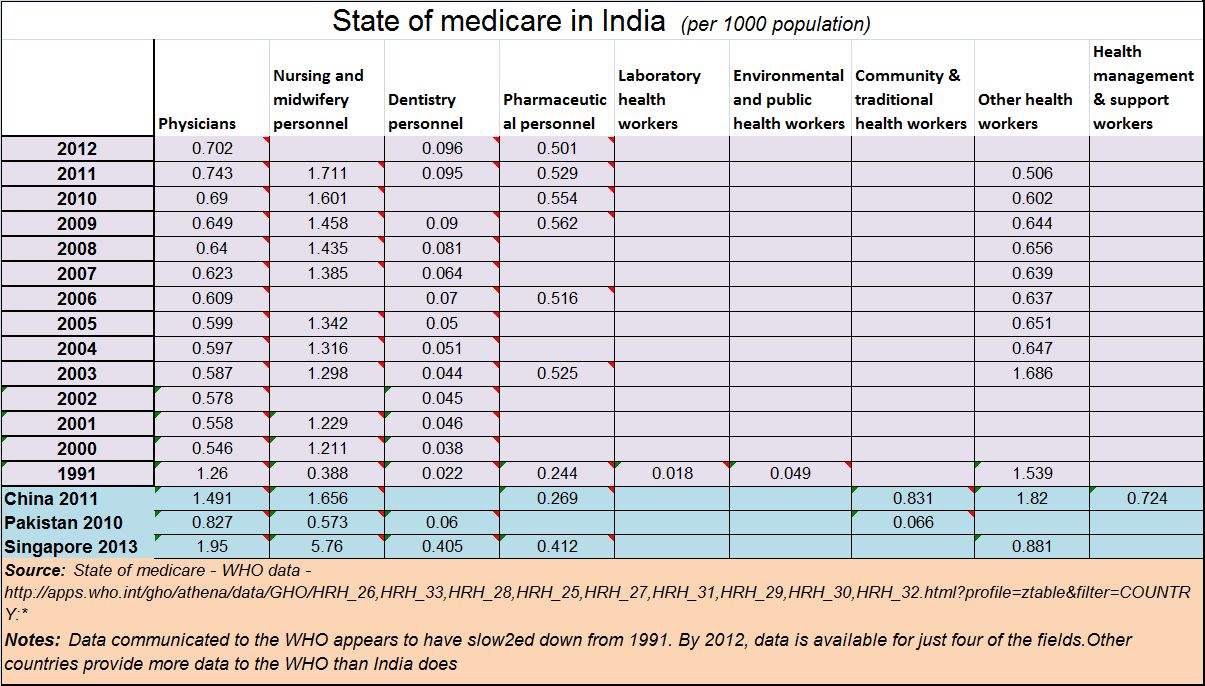 Some other neighbouring countries, including Pakistan, appear to be doing a better job in data compilation and communication than India does.
Some other neighbouring countries, including Pakistan, appear to be doing a better job in data compilation and communication than India does.
One reason could be that India does not like to collect, or disseminate, inconvenient data. Consider for instance the way India did not even bother to collect and compile much of the data on the people who died each year (http://www.asiaconverge.com/2015/10/does-anybody-care-for-the-dead/). Data gleaned from the Report on Medical Certification of cause of Death 2010, Office of the Registrar General of India, Govt. of India, shows that India registers data on just 2.86% of the people who actually die each year. In other words, 85.7% of deaths go unrecorded. It was only in August 2014 that the Registrar General formally raised this issue and has begun working on ways to ameliorate the situation. .
Similarly, consider the manner in which data on education is fudged (http://www.asiaconverge.com/2016/12/fudging-education-data-produces-sludge/)
But there are other signs of disdain for processes. Even after 70 years after independence, India has yet to lay down norms for diagnostics. There are no standard norms prescribed by the government for pathology. Therefore, each pathology laboratory analyses blood, urine or stool (or anything else) according to the parameters supplied by the manufacturers of the equipment they have installed in their clinics. Each pathology laboratory informs doctors of the range that should be considered normal. There is just no national standard.
Take a third malaise. India does not even respect professionalism in medical education. In Maharashtra, the state government had the brazen audacity to pass an order that homeopaths could legally practice (the globally accepted) allopathic lines of treatment. Everywhere in the world, medical colleges generally train students along the lines prescribed by allopathy. Institutions teaching students homeopathy are clearly described as being nothing more than homeopathy colleges. Ditto for Ayurvedic colleges, or institutes teaching or practicing Chinese traditional medicine. While all these sciences do study the human body and its ailments, and ways to cure them, the approaches towards treatment and cure are different. A student trained in one stream is not considered competent to practice another stream without passing a qualifying exam.
Instead, Maharashtra has been trying to allow homeopaths to be equated with allopaths possibly because then the demand for admission to homeopathic colleges would increase. Allopathy offers greater scope for moneymaking. That could also explain why most private medical, engineering and homeopathy colleges in this state are run by organizations perceived to be very close to politicians.
The Indian Medical Association has challenged the attempts to equate homeopaths with allopaths. The matter awaits a judicial verdict. But more on this later.
That also explains the extreme reluctance on the part of most state governments and even municipalities to having a computerized system which logs in details of treatment given to individuals and the medicines prescribed and dispensed. It would go a long way towards creating a data bank of health services and medicines purchased and dispensed. It is only recently that Mumbai has decided to go ahead with such computerization. One hopes that other cities and states also do this.
The absence of data and standards in medicare has made all policy making in this vital area extremely whimsical and difficult. Lobbies push their version to the ministry concerned, and the ministry then churns out (often specious) reasons justifying the acceptance of new norms. The same capriciousness then spreads to the Food and Drug Administration (FDA) which too comes up with arbitrary demands, prescriptions and penalties. The FDA – it may be recalled — has been hauled up by the Supreme Court quite sharply in the Nestle matter in October 2015 (http://www.asiaconverge.com/2015/10/food-drugs-ban-leads-to-caprice-and-corruption/).
All these aberrations, and the casual approach towards record keeping, have contributed to the blanks in the data that is submitted by India to the WHO.
Will the government address this problem? Or will it allow India to draft aimlessly the way many countries on the African subcontinent have?
One hopes and prays that the former will prevail.






{kind=link}
COMMENTS